|
Neuroimaging of central nervous system tuberculosis
Authors:
Catarina Granjo Morais, 1 , Ana Reis Melo, 2 , Joana Oliveira, 3 , Augusto Ribeiro, 4 , Irene Pinto Carvalho, 1 , Margarida Tavares, 2 ,
1 Department of Pediatrics, Centro Hospitalar e Universitário São João, Porto, Portugal
2 Pediatric Infectious Diseases and Immunodeficiency Unit, Department of Pediatrics, Centro Hospitalar Universitário São João, Porto, Portugal
3 Department of Neurosurgery, Centro Hospitalar e Universitário São João, Porto, Portugal
4 Pediatric Intensive Care Unit, Centro Hospitalar e Universitário São João, Porto, Portugal
Corresponding Author:
Catarina Granjo Morais
keywords: tuberculosis
Abstract
A 20-month-old female, not immunized with Bacillus Calmette-Guérin (BCG) vaccine, was admitted due to a four-day history of fever and cough. In the past three months, she presented respiratory infections, weight loss and enlarged cervical lymph nodes. On day two of admission, she displayed drowsiness and positive Romberg’s sign; cerebrospinal fluid (CSF) workout revealed 107/ul cells, low glucose and high protein levels. Ceftriaxone and acyclovir were initiated, and she was transferred to our tertiary hospital. Brain magnetic resonance imaging showed punctiform focal areas of restricted diffusion in left capsular lenticular region suggestive of vasculitis secondary to infection. Tuberculin skin test and interferon-gamma release assay were positive. She started tuberculostatic therapy, but two days later she presented tonic-clonic seizures and impaired consciousness. Cerebral computed tomography (CT) revealed tetrahydrocephalus (Figure 1), needing external ventricular derivation. She had a slow clinical improvement, requiring several neurosurgical interventions and developing a syndrome of inappropriate antidiuretic secretion alternating with cerebral salt wasting. Positive results for Mycobacterium tuberculosis were obtained by CSF culture and by polymerase chain reaction in CSF, bronchoalveolar lavage and gastric aspirate specimens. Repeated brain CT showed a large-vessel vasculitis with basal meningeal enhancement, typical of central nervous system (CNS) tuberculosis (Figure 2). She completed one month of corticosteroids and maintained antituberculosis treatment. At two years of age, she has spastic paraparesis and no language skills.
Portugal had 1836 cases of tuberculosis (17.8 per 100000) in 2016 and was considered a low-incidence country; consequently, BCG vaccination is not universal (1). We present a severe case of CNS tuberculosis with intracranial hypertension, vasculitis and hyponatremia, associated with poorer outcomes (2). A high index of suspicion allowed prompt start of antituberculosis treatment. Diagnosis was corroborated by microbiological positivity and a typical triad in neuroimaging (hydrocephalus, vasculitis and basal meningeal enhancement) (3), which we wish to emphasize.
Acknowledgement:
The authors have no acknowledgements to declare.
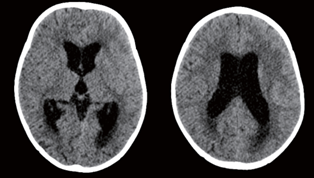
Figure 1. Acute hydrocephalus - ventricular dilatation and periventricular white matter edema due to the transependymal resorption of spinal fluid (occipital horn of the lateral ventricles).
.png)
Figure 2. Large-vessel vasculitis involving bilateral frontobasal and frontal parasagittal, right temporo-occipital corticosubcortical areas and left lenticulocaudate. It is also noticeable the basal meningeal enhancement typical of central nervous system tuberculosis.
REFERENCES
- Leite Tuberculous Meningitis - An Entity Not to Forget. Neonatology and Clinical Pediatrics. 2021;8(1):1-4.
- Muzumdar D, Vedantam R, Chandrashekhar Tuberculosis of the central nervous system in children. Childs Nerv Syst. 2018;34(10):1925-35.
- Kritsaneepaiboon S, Andres MM, Tatco VR, Lim CCQ, Concepcion Extrapulmonary involvement in pediatric tuberculosis. Pediatr Radiol. 2017;47(10):1249-59.
|