Purpose: Minor injury to head and neck is usually neglected for potential neurological consequences. We report a woman who suffered left Eagle syndrome due to styloid process fracture two years after a minor motorcycle collision.
Case Report: A 53-year-old woman complained pain at her left upper neck, lower face and periauricular area after minor motorcycle collision at 2 years ago. The pain usually occurred spontaneously but was occasionally triggered or exacerbated by specific postural changes, including looking up or turning head to right side. Moreover, a foreign body sensation occurred at throat during swallowing. Physical examination provoked pain at the left submandibular area. Carotid bruit was absent. Otherwise, other neurological function was preserved. Computerized tomography revealed linear fracture at the middle of left styloid process. After inform, patient preferred conservative treatments including abortive non- steroidal anti-inflammatory drugs and an avoidance of rapid head rotations. Since afterwards, the frequency and intensity of neck pain greatly decreased and she could tolerate and maintain a normal daily living.
Conclusions: Asymptomatic or paucisymptomatic styloid process fracture may be neglected in case of minor injury to head and neck. A careful evaluation of neck should be completed in traumatic individuals to reveal underlying damage and prevent further harmful consequence.
Keywords: Eagle syndrome, styloid process, pain, head injury.
INTRODUCTION
Motorcycle is still the most common traffic vehicle in Taiwan and other developing Asian countries because of convenience and economic. Minor falling accident is frequent. The incidence of traumatic brain hemorrhage dramatically decreased since the introduction of helmet use and alcohol drink prohibition in Taiwan (1,2). Delayed onset of minor head and neck injury, however, may be overlooked in clinical practice. We present a woman who suffered a minor motorcycle collision complained left neck pain since afterwards. Fractured styloid process (SP) of the temporal bone was found.
CASE REPORT
A 53-year-old woman complained a progressive deterioration of pain at her left upper neck, lower face and periauricular area after minor motorcycle collision, that she fell on left side to ground about 2 years ago. Patient emphasized to have worn her helmet at that time. The pain usually occurred spontaneously but was acutely exacerbated by specific head movements, including looking up or turning head to right side. Moreover, patient described a foreign body sensation at throat during swallowing. Left tinnitus (ill-defined non-staccato sound) was also present. Physical and neurological examination provoked pain at the left submandibular area over the anterior border of sternocleidomastoid muscle. Mouth opening or closing did not exacerbate this index pain. Carotid bruit was absent. Radial pulsation was symmetry. Otherwise, no abnormal finding was documented. Previous personal or medical history was not contributable. Skull radiology did not clearly show strong morphological change of left styloid process. The 3D computerized tomography was arranged and revealed fracture at the middle of left SP of the temporal bone (Fig. 1 A & B). The length of SP was around 3.1 cm at right side whereas also 3.1 cm (1.2 cm and 1.9 cm of the two fractured process, respectively) at left side. After inform of treatment policies, patient decided to receive conservative treatments, that included abortive non-steroidal anti- inflammatory drugs and an avoidance of rapid head rotations to prevent pain triggering. On the follow-up period, the frequency and intensity of neck pain greatly decreased but was not completely exiled. Patient could tolerate and maintain a normal daily living.
DISCUSSION
Our patient suffered a consistent pain at the submandibular area and episodic pain at her left face and neck on neck and head rotation, that was compatible with Eagle syndrome (3), which consisted of two distinct cluster of syndromes (4). The classical styloid syndrome is characterized by the pain localized in the tonsillar fossa probably resulting from an involvement of cranial nerves V, VII, VIII, IX, or X by elongated SP or calcified styloid ligament. Other symptoms include dysphagia, odynophagia, and foreign body sensation in the throat. In occasions, pain may occur at temporomandibular area mimicking temporomandibular disorder. Styloid-carotid syndrome, or vascular Eagle syndrome, is characterized by vascular compromise of the internal or external carotid artery in that is usually caused by a laterally or medially deviated styloid process. The clinical manifestation of fractured SP (5,6) is poorly understood between with Eagle syndrome and is doubted if the floating fractured SP might
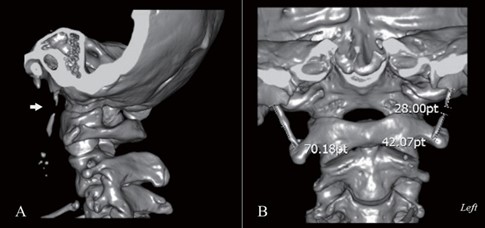
Figure 1. 3D computerized tomography revealed fracture at the middle of left styloid process of temporal bone in our patient (arrow) (A). The length of SP was around 3.1 cm at right side and also 3.1 cm at left side (1.2 cm and 1.9 cm of the two fractured process, respectively) (B).
provoke protean deficits rather than a consistent pain character. Similar to our patient, fractured SP surprisingly elicited painful events resembling non-fractured SP reported in literature (4-7). The styloid ligament and confined lateral pharyngeal space may anchorage and limit the movement of the fractured SP to elicit more extensive damage. Importantly, fractured SP may cause devastating complication (8) despite of a benign outcome in ours and previous reports. Till now, the frequency of symptomatic or asymptomatic SP fracture is unknown. The single report included 84 patients with maxillofacial trauma in that 27 patients of them (32.1%) were found to have concomitant symptomatic SP fracture (6). Therefore, appropriate styloid examination should not be neglected in whom lateral neck pain ensues for minor head/neck trauma.
Eagle syndrome usually occurs in men, middle age, and with elongated SP or calcified styloid ligament (4). On the other hand, the frequency of symptomatic fractured SP is similar in either gender in maxillofacial trauma (6), and that virtually reflects a similar frequency of head trauma events in population. The shaft of SP embryologically originates from the stylohyal part of Reichert's cartilage and undergoes endochondral ossification until at 8 years of life. Since menopause generally associates with a reduction of bone density and increases the risk of bone fracture in women, it is expected to risk for SP fracture superimposing with biomechanical stress as in our patient. Nevertheless, a presence of associated risk of fracture, such as menopause or previous history of fracture, should alert for SP fracture after minor neck/face injury.
Our patient did not have any neck/face discomfort before until after index injury. The length of SP was 3.1 cm at both normal and fractured side. The average length of SP is 2.0-2.5 cm in human in previous studies (5). Elongation of SP is defined as the length of SP to be more than 3.0 cm (9) and is found in 4% in population (5). Generally, painful symptoms relate to the length of SP, angle of deviation and calcification of stylohyoid ligament, as well as unique head/neck posture (2). It is not surprising that our patient did not have any painful symptom before as only 4%-10% of elongated SP persons manifests responsible head/neck pain (5,10). Therefore, stressful fracture is postulated to trigger the painful event in our patient. If so, we would like to propose that incidental trigger seemingly predisposes to painful attacks in Eagle syndrome patients with elongated SP when painful event occurs mostly after 40 years in and high prevalence of asymptomatic elongated SP persons (11).
The clinical history and findings of our patient provide that fractured SP should be alerted for persons who suffered traumatic event even though they claimed to have full protection of their head, such as helmet use, and did not initially experience symptomatic concussion syndrome. Incidental trigger may predispose for Eagle syndrome in elongated SP persons.
ACKNOWLEDGEMENT
This study has been approved by the Chang Gung Medical Foundation Institutional Review Board (IRB code: 202000821B0).
REFERENCES
1. Chiu WT, Yeh KH, Li YC, Gan YH, Chen HY, Hung CC. Traumatic brain injury registry in Taiwan. Neurol Res 1997;19:261-4.
2. Chiu WT, Huang SJ, Tsai SH, Lin JW, Tsai MD, Lin TJ, Huang WC. The impact of time, legislation, and geography on the epidemiology of traumatic brain injury. J Clin Neurosci 2007;14:930-5.
3. Eagle WW. Elongated styloid process. Report of two cases. Arch Otolaryngol 1937; 25:584-587.
4. Badhey A, Jategaonkar A, Anglin Kovacs AJ, Kadakia S, De Deyn PP, Ducic Y, Schantz S, Shin E. Eagle syndrome: A comprehensive review. Clin Neurol Neurosurg 2017;159:34-8.
5. Khan HM, Fraser AD, Daws S, Thoppay J, Mupparapu M. Fractured styloid process masquerading as neck pain: Cone-beam computed tomography investigation and review of the literature. Imaging Sci Dent 2018; 48:67-72.
6. Tiwary P, Sahoo N, Thakral A, Ranjan U. Styloid process fracture associated with maxillofacial trauma: Incidence, distribution, and management. J Oral Maxillofac Surg 2017;75:2177-82.
7. Kermani H, Dehghani N, Aghdashi F, Esmaeelinejad M. Nonsyndromic isolated temporal bone styloid process fracture. Trauma Mon 2016;21:e24395.
8. Arechvo I, Giniunaite AM, Balseris S. Bilateral fracture of the styloid process with parapharyngeal emphysema. Otol Neurotol 2014;35:e155-e156.
9. Custodio AL, Silva MR, Abreu MH, Araújo LR, de Oliveira LJ. Styloid process of the temporal bone: M orphometric analys is and clinical implications. Biomed Res Int 2016;2016:8792725.
10. Rechtweg JS, Wax MK. Eagle's syndrome: a review. Am J Otolaryngol 1998;19:316-21.
11. Sridevi K, Mahesh N, Krishnaveni B, Deepika ADN, Thejasri V, Leninson BHD. Evaluation of styloid process and its anatomical variations: A digital panoramic study with systematic review. J Int Soc Prev Community Dent 2019;9:256-62.